Clinical Alarm Management & Notification Systems
Clinical monitoring devices and sensors used within the alarm notification system, including Root, Radius VSM, and supporting instruments
UX Design Lead, Clinical Notification Systems & Instruments - Led design for alarm routing, assignment workflows, and device-state behavior. Defined a state-driven alarm management system across bedside devices and clinical dashboards, reducing unnecessary alerts and improving response accuracy in high-acuity environments.
Operational Outcomes
Reduced alarm interruptions per shift from 115 to 35
Improved response time by approximately 20%
Increased assignment accuracy by approximately 15%
System Design & Logic
The Patient SafetyNet ecosystem coordinates patients, monitoring devices, and care teams through a shared notification infrastructure. Each component operates independently but must remain synchronized to ensure alarms are routed to the correct caregiver in real time.
Whiteboarding core assignment logic, including patient admission, assignment updates, and audit states
Core Relationships
Patients are assigned to respondents
Devices are associated with patients
Alarm routing depends on assignment state and configuration
Notification delivery depends on responder availability and device readiness
State-Driven Behavior
Assignment: assigned, unassigned
Device: docked, undocked, transferring, standby
Alarm: triggered, suppressed, escalated, resolved
Clinical Context & Systemic Causes of Alarm Fatigue
Initial hospital data revealed a high volume of alerts generated from expected device behavior rather than true clinical events. Many alarms were triggered during routine workflows such as sensor disconnections, patient transfers, low battery states, and temporary signal interruptions, contributing to unnecessary noise and reduced signal clarity.
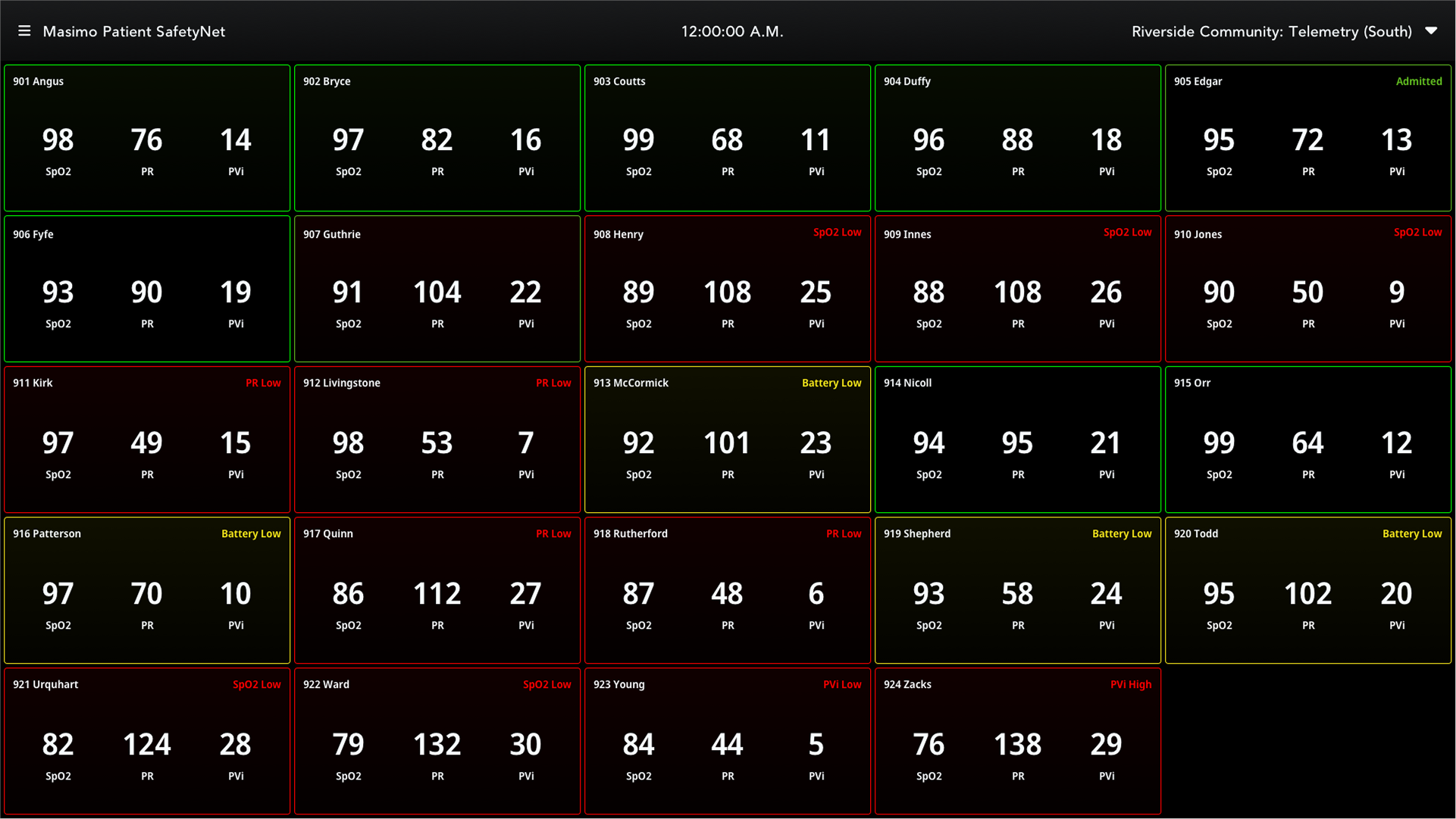
Patient SafetyNet View Station showing multiple patient states alongside physiological and technical alarms across the unit
Insights from Field Observation & Hospital Visits
Misrouted alarms due to incorrect or outdated assignments
Inaccurate nurse assignments impacting notification delivery
Alarms triggered during expected device states (e.g. transfer, disconnection)
High volumes of non-actionable alerts
Assignment Management
Assignment management was a multi-step process that required significant cognitive effort and time to complete. In practice, no hospital floors achieved 100% assignment accuracy, and there was no scalable way to audit or verify assignments.
Assignments were often completed under time pressure during shift changes, leading to incomplete or outdated configurations. In some cases, caregivers did not use their assigned pagers, further contributing to misrouted alarms and gaps in notification coverage.
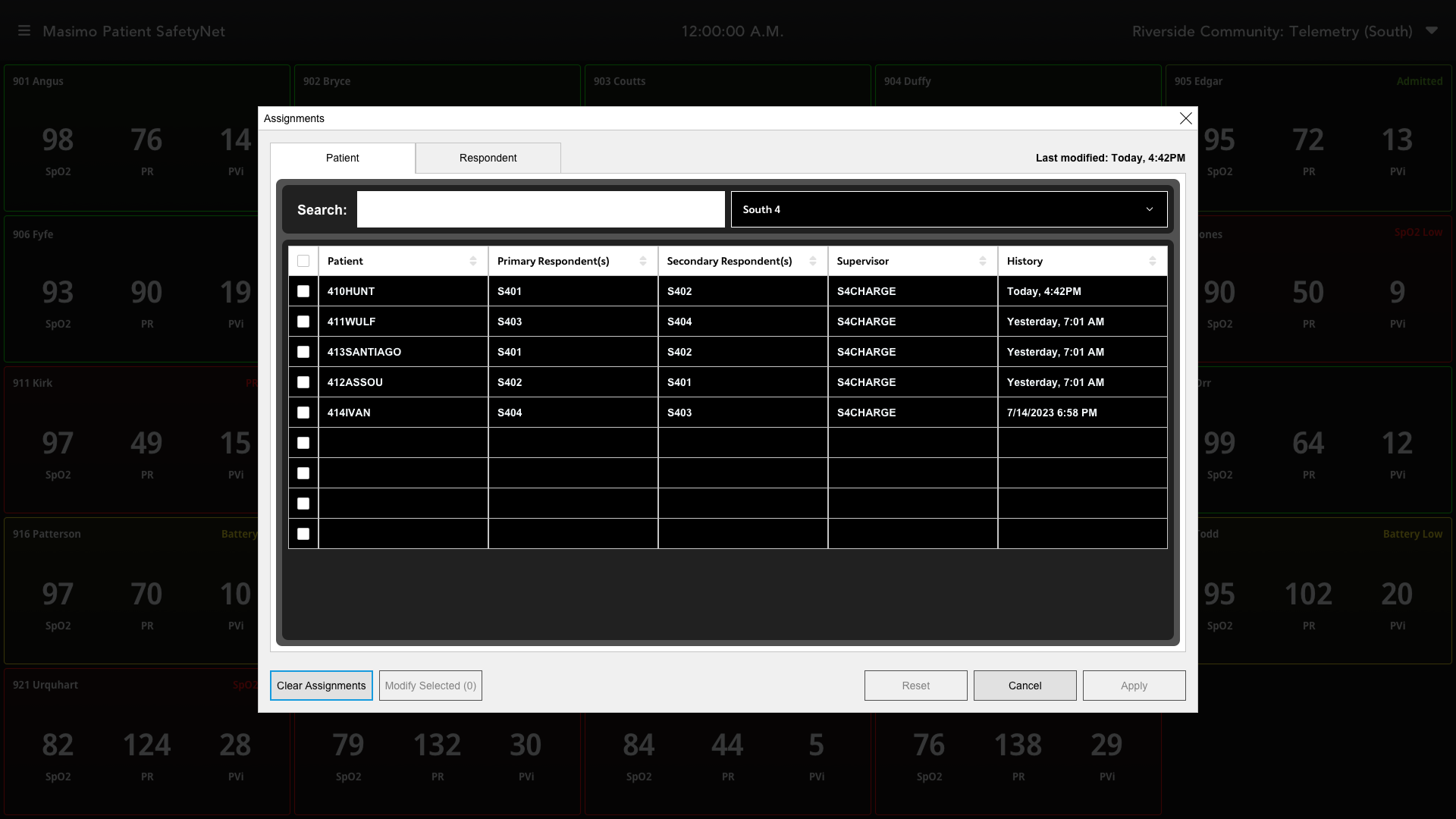
New assignment interface featuring audit history, last modified timestamps, clear assignments, and bulk assignment capabilities
Workflow Redesign
Reduced steps to streamline assignment creation and updates
Surfaced errors earlier in the process
Introduced patient-centric and respondent-centric views
Enabled quick search, clear/reset at shift boundaries, and conditional apply
Improved Assignment Accuracy
Reduced clicks and cognitive load
Increased assignment accuracy across clinical teams
Improved clarity of responsibility, ensuring alarms reached the correct caregivers
Alarm Routing & Notification Domains
Misrouted alarms increased clinical risk by broadcasting alerts too broadly across care teams. Notifications were often sent to clinicians who were not responsible for the patient or best equipped to respond, leading to unnecessary interruptions and delayed response times.
Alarms were not aligned to specific roles. Low battery alerts, for example, could be routed to a biomedical technician, while respiratory-related alarms such as SpO₂ and respiration rate should be directed to respiratory therapists. Without role-based routing, alerts were frequently misdirected.
Routing Alarms to the Correct Clinical Roles
Linking routing directly to nurse assignments
Introduced configurable notification domains
Enabled role-based responder assignment
Improved Response Times
Reduced unnecessary interruptions
Improved signal-to-noise ratio
Enabled faster, more reliable responses
Role-based notification assignments enabling targeted alarm routing across care teams
Device Transfers
False alarms were frequently triggered during expected device states, particularly during intentional sensor disconnections. During device transfers, the system interpreted these transitions as true sensor disconnect events, generating unnecessary alarms.
Because device transfers occurred regularly, these alerts contributed significantly to overall alarm volume, disrupted clinical workflows, and skewed monitoring analytics by recording non-actionable events as real incidents.
Standby Mode & Transfer Automation
Automatically triggered standby when Radius VSM was undocked from Root
Suppressed alarms during transfer states
Preserved monitoring configurations (e.g., NIBP scheduling) across devices
Added manual standby and patient disassociation controls
Reduced Alarm Noise & Improved Workflow
Eliminated unnecessary alarms during transfers
Reduced clinician frustration
Improved accuracy of monitoring analytics

Device enters a standby state during transfer, suppressing false alarms triggered by expected sensor disconnections
Outcomes and Impact
Baseline (Observed in Clinical Environments)
7,145 total notifications across monitored units
~115 notifications per shift in high-volume environments
Impact
Reduced non-actionable alarm noise by ~30%
Improved assignment accuracy by ~20%
Reduced response time to critical alarms by ~15-20%
Eliminated false alarms during device transfers (~90% reduction)
* Estimates based on observed system behavior and field testing in clinical environments.